Lp(a) and Genetically Linked Coronary Artery Disease
 Lp(a) is a nasty form of LDL that does plenty of damage in the body. Many people with a family history of heart attacks can point to this lipid. Read more to learn about it, get tested for it, and lower your risk.
Lp(a) is a nasty form of LDL that does plenty of damage in the body. Many people with a family history of heart attacks can point to this lipid. Read more to learn about it, get tested for it, and lower your risk.
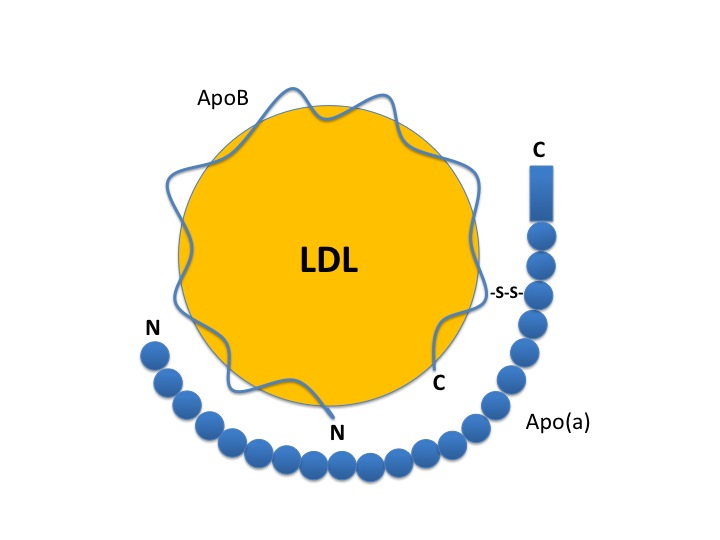
Let’s use this analogy to describe Lp(a). LDL is like a baseball. Apo B-100 is the stitching of the baseball. Pretty normal so far. Apo (a) is similiar to little spikes on the stitches. Doesn’t sound so fun to play anymore. Again, this is a dangerous LDL particle.
Apo B-100 is a protein on the surface of all VLDL and LDL particles. It plays a major role in docking of the LDL to cells around the body.
Lp(a) plasma concentrations are controlled by the apo(a) gene. This may be a major source of genetically linked coronary artery disease.
Lp(a) looks like plasminogen, a protein involved in clot prevention. This similarity likely leads to the inability of the body to dissolve clots and increased heart attack risk. Lp(a) also recruits inflammatory cells to the blood vessel wall, leading to plaque formation and rupture. The Lp(a) is easily oxidized leading to intracellular cholesterol accumulation. Lp(a) appears to interfere with blood vessel dilation.
The oxidized Lp(a) and the glycated Lp(a) have a much more potent effect than native Lp(a) in promoting the development of atherosclerotic disease. Oxidation happens to lipids from poor nutrition and chemicals. Glycation is a change to lipids from elevated blood sugar.
Mechanisms of Lp(a) damage:
1) Avidly taken up by inflammatory cells in plaque
2) Leads to inflammatory cell recruitment to plaque
3) Interferes with plasminogen therefore clot breakdown
4) Impairs vasodilation
5) Promotes smooth muscle cell proliferation
6) Impairs barrier function of endothelial cells
Elevated serum Lp(a) is an independent predictor of coronary artery disease, myocardial infarction, and stroke. Lp(a) levels are a marker of restenosis after percutaneous transluminal coronary angioplasty, saphenous vein bypass graft atherosclerosis, and accelerated coronary atherosclerosis of cardiac transplantation. Serum Lp(a) levels ≥ 25mg/dL are noted in 67% of patients with rapid progression of coronary artery disease but in only 33% of patients without progression of coronary artery disease.
The Copenhagen City Heart Study found that extreme Lp(a) levels > 95th percentile predict a 3- to 4-fold increase in risk of myocardial infarction and absolute 10-year risks of 20% and 35% in high-risk women and men.
Lp(a) blood levels can be a difficult molecule to lower, but interestingly, saturated fat intake decreases levels by 10%. Trials using statin therapy have not shown any consistent benefit. Hormone replacement therapy in women has proven effective. Time-release niacin lowers levels by 20-30%. N-acetyl cysteine, vitamin C, and L-carnitine also have promising data. Because of the increased clotting risk associated with Lp(a), it is my personal recommendation to use nattokinase or lumbrokinase along with marine omega 3 oils, mixed tocopherol vitamin E, and garlic.